ACE inhibitors (angiotensin-converting enzyme inhibitors) are a type of medicine that is mostly used to treat hypertension and heart diseases by relaxing blood vessels. ACE inhibitors blocks the activity of angiotensin-converting enzyme, which do not allow the conversion of angiotensin 1 into angiotensin 11. Moreover it also increases the levels of a peptide bradykinin that lowers blood pressure by opening blood vessels.
All of the ACE inhibitors are available in oral dosage form except enalapril, that is available oral & intravenous injectables. FDA has approved ten angiotensin-converting enzyme inhibitors till date . Captopril was the first approved in 1981 by FDA for hypertension. Others are Enalapril, Lisinopril, Ramipril, Trandolapril, foscinopril, perindopril, quinapril, benazepril moexipril.
On the basis of the chemical structure, angiotensin-converting enzyme inhibitors can be classified into three groups. yjat are
Sulfhydryl-containing ACE inhibitors (Captopril)
Phosphorus-containing ACE inhibitor (Fosinopril)
Dicarboxylic-containing ACE inhibitors (Enalapril, Lisinopril etc)
Mechanism of action
Primary mode of action of angiotensin-converting enzyme inhibitors involves the suppression of the angiotensin-converting enzyme (ACE), which is necessary for the renin-angiotensin-aldosterone system.
ACE inhibitors (angiotensin-converting enzyme inhibitors) blocks the conversion of angiotensin I angiotensin II. Angiotensin II is a strong vasoconstrictor that elevates blood pressure by making blood vessels smaller.
ACE inhibitors controls blood pressure and enables the heart to work less by reducing the levels of angiotensin II. The reduced levels of angiotensin II opens up blood vessels, lowers blood pressure and makes the heart work less.
ACE inhibitors (angiotensin-converting enzyme inhibitors) also lowers the secretion of aldosterone from adrenal glands. It makes the body hold onto less sodium and water and lowers blood volume and pressure.
ACE inhibitors also inhibits the metabolism or breakdown of a peptide named bradykinin that lowers blood pressure by opening blood vessels. However the higher levels of bradykinin may create side effects like hypotension, dry cough, electrolyte imbalance or angioedema. Many drugs belong to this group. however differ a little in mechanism of action, the side effects they cause. All work much the same to lower blood pressure and protect the heart and kidneys.
Indications
For the treatment of high blood pressure in adults the Eighth Joint National Commission (JNC8), published evidence-based guidelines in 2014. These guidelines recommended ACE inhibitors as one of the four drug classes that can be used as initial therapy in hypertension.
According to the American Heart Association/American College of Cardiology (AHA/ACC) and the European Society of Cardiology (ESC) guidelines 2023, angiotensin-converting enzyme inhibitors can be used as first-line antihypertensive protocol, preferably for the patients suffering with chronic cardiovascular diseases & diabetes mellitus.
ACE inhibitors reduces the progression of disease nephropathy in Type 1 (insulin-dependent diabetes mellitus) and greatly lower the risk of death, dialysis, and transplantation.
ACE inhibitors stop microalbuminuria from getting worse and turning into overt proteinuria. They also stabilize kidney function in people who have never been treated before and have compromised kidney function.
Heart attack or myocardial infarction
left ventricular systolic dysfunction
Adverse Effects
Common Adverse Effects; Dry cough, headache, fatigue, weakness, diarrhea, nausea, dizziness, Hypotension
ACE inhibitor-induced dry non productive cough is more common among women than men.
Reduced glomerular filtration rate GFR, & higher serum creatinine is observed in approximately 30%. It become more significant when diuretics and NSAID s are administered along with ACE inhibitors (angiotensin-converting enzyme inhibitors).
One-fifth of the patients suffering with renal artery stenosis may develop elevated levels of BUN in blood urea nitrogen and creatinine levels. This decline in renal function is reversible & stabilizes within 2-4 weeks.
Angioedema, most significant adverse effect that can affect any part of the body however tongue, glottis or larynx mostly effected & cause airway obstruction. Rate is high in African-American population. Many drugs like epinephrine. diphenhydramine, methylprednisolone & bradykinin blocking agents can be used. However in case of airway compromise , the airway along with an endotracheal tube is applied that allows ventilation.
Hyperkalemia especialy
Cholestatic jaundice or hepatitis or hepatic necrosis in rare cases
Although the efficacy of Angiotensin receptor blockers (ARBs) & ACE inhibitors are similar but later has a higher incidence of side effects like cough and angioedema. this is the reason that some clinicians prefer to prescribe ARBs. over angiotensin-converting enzyme inhibitors.
Hematologic disorders like neutropenia, agranulocytosis and other blood dyscrasias may occur.
Precautions to use ACE inhibitors (angiotensin-converting enzyme inhibitors)
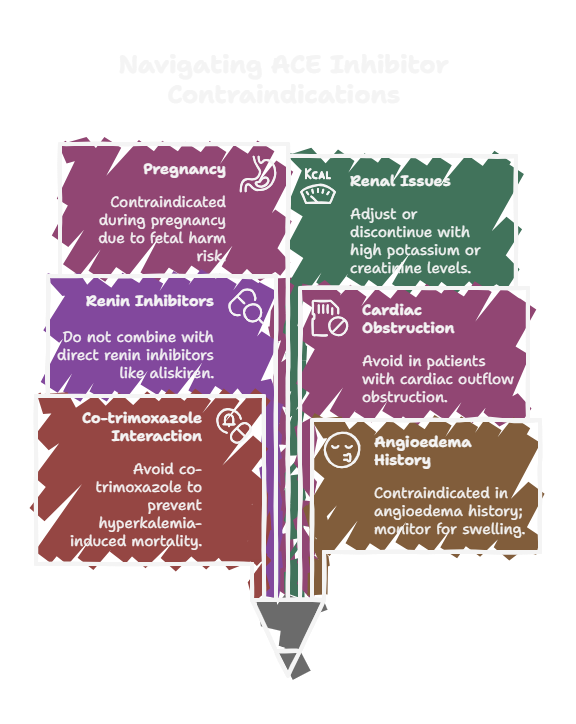
Concomitant administration of ACE inhibitors and co-trimoxazole may cause mortality (sudden death) due to hyperkalemia.
ACE inhibitors are contraindicated in patients with a history of angioedema or hypersensitivity. Monitor if signs of angioedema appear, like swelling of the face, lips, tongue, or throat, stop its use & seek immediate medical attention.
It should not be given to patients already taking a direct renin inhibitor such as aliskiren.
It should not be given to patients cardiac outflow obstruction
It should not be given to patients with hypovolemia or dehydration
ACE inhibitors should not be given during pregnancy due to the risk of fetal harm as it may cause congenital malformations, neonatal death or still birth, . Women planning to conceive or who become pregnant should consult physician prior use.
The combination therapy of ACE inhibitors with other antihypertensive drugs especially ARBs & potassium-sparing diuretics can worse renal indices, hypotension and life-threatening hyperkalemia.
Avoid if you have a known allergy to ACE inhibitors.
High potassium levels or creatinine or decreased glomerular the drug needs to be adjusted accordingly or discontinued.
Dosage form & Dose
All of the ACE inhibitors are available in oral dosage form except enalapril, that is available oral & intravenous injectables. FDA has approved ten angiotensin-converting enzyme inhibitors till date . Captopril was the first approved in 1981 by FDA for hypertension. all have some differences regarding its uses , mechanism or side effects but they all work the same to decrease blood pressure and protecting the heart and kidneys. Some doses of ACE inhibitors for hypertension are as follow
Captopril: Tab 25 mg. start dose 12.5–25 mg bid-tid with a maximum daily dose of 150mg
Enalapril: Tab 5 mg. initial dose 5 mg , a maximum daily dose of 40 mg
Lisinopril: Tab 10 mg. initial dose 10 mg , a maximum dose of 80 mg
Benazepril: Tab 10 mg. initial dose 10 mg , a maximum dose of 80 mg
Ramipril: Tab 2.5 mg. starting dose 2.5 mg , a maximum dose of 20 mg
Trandolapril: Tab 2 mg. starting dose 1 mg , a maximum dose of 8 mg
Quinapril: Tab 10 mg. starting dose 10 mg , a maximum dose of 80 mg
Perindopril: Tab 4 mg. starting dose 4 mg , a maximum dose of 16 mg
Moexipril: Tab 7.5 mg. initial dose7.5 mg , a maximum dose of 30 mg
Fosinopril: Tab 10 mg. initial dose 10 mg , a maximum dose of 80 mg
Ramipril is normally preferred since there is a lot of evidence that it helps to manage hypertension if the heart and kidneys are compromised. it is used in various of conditions and it is linked to a lower risk of death.
Lisinopril and enalapril are prevalent in practice because they are easy to get and have a lot of evidence behind them, although they may have more side effects, such as persistent cough.
Captopril is less convenient as it needs to be taken many times a day. Preference to prescribe rely on many factors like patient variables, side effect profiles, cost & availability.
Conclusion
ACE inhibitors (angiotensin-converting enzyme inhibitors) reduce blood pressure and safeguard the heart and kidneys by inhibiting the production of angiotensin II and enhancing bradykinin levels. Captopril & Ramipril are frequently regarded as the preferred ACE inhibitors due to wide range of indications and best outcomes; however, selection may differ according to specific patient characteristics and side effect profiles. Angiotensin receptor blockers (ARBs) are often taken as alternatives because of improved tolerability while maintaining same therapeutic efficacy.