Alpha-Blockers
Alpha-blockers are also recognized as α-adrenergic receptors antagonists. It is a class of medications that work by blocking the effects of norepinephrine and epinephrine on alpha-adrenergic receptors. Alpha blockers relax blood vessels, improve blood flow, that help to lowers high blood pressure and prostate issues. Alpha receptors are found in various parts of the body, mainly in the smooth muscles of blood vessels, the prostate, and the bladder. They reduce blood pressure by expanding the cardiovascular system’s blood vessels. They make the bladder neck wider in the urinary tract to help urine flow better and get rid of any blockage that could be caused by an enlarged prostate or a kidney stone. Alpha blockers begin to work immediately, but the best results appear in four to six weeks of use. What is the mechanism of action of Alpha blockers. Alpha-blockers competitively inhibit the affinity of adrenaline & nor adrenaline to the alpha-adrenergic receptors. Adrenaline or nor adrenaline are released from adrenal glands, cause vasoconstriction and their inhibition lead to vasodilatation. There are two main subtypes of alpha-receptors: Non-Selective Alpha-Blockers: these drugs act on both alpha-(α1and α2) receptors and block their activity. Although these drugs are effective vasodilators, however less commonly indicated for hypertension treatment to side effects like reflex tachycardia and high sympathetic activity. They are mainly prescribed for specific conditions for a short time. Phenoxybenzamine and Phentolamine belongs to this group. α1 receptors; These receptors are located throughout the body, mainly at the neck of bladder, smooth muscle cells in the walls of peripheral blood vessels & the prostate. Alpha-blockers widen the blood vessels and produce vasodilation by blocking these receptors. These drugs improve urine flow by the relaxation of the bladder neck and prostate. they are of three types named as α1A receptors, α1B receptors, α1D receptors. Prazosin, Terazosin, Doxazosin, Tamsulosin, Alfuzosin, Silodosin belongs to this group. α2 receptors: These receptors are located on nerve terminals and other tissues. Selective α1 receptors blocker are most commonly used alpha-blockers that minimize the side effects associated with the blocking of α2 receptors. Indications Alpha-blockers are mainly used to treat two main disorders Benign Prostatic Hyperplasia (BPH): Alpha-blockers are drug of choice for benign prostatic hyperplasia. BPH is due to the enlargement of the prostate gland with the symptoms like weak stream, frequent urination & dribbling. These drugs relax the smooth muscles, make the bladder neck wider in the urinary tract to help urine flow better and get rid of any blockage that could be caused by an enlarged prostate or a kidney stone. Hypertension (High Blood Pressure): Although it is not the first choice or protocol, however in complex cases can be used along with other drugs. Alpha-blockers lower peripheral resistance by relaxing blood vessels that in turn lowers blood pressure. Pheochromocytoma It is a rare disease of the adrenal gland having tumor, that secretes excessive amount of epinephrine and norepinephrine. Excessive release of catecholamines immensely raise blood pressure. Alpha-blockers are considered the first choice for managing hypertension in patients with pheochromocytoma, especially before surgery for the removal of tumor. alpha blockers block the effects of the excess hormones and prevent life-threatening hypertension during the surgical procedure. Raynaud’s disease: It is a rare disease in which vasospasms occur mostly in the fingers and toes due to stress or cold. The drugs of this class can be used to reduce the frequency and severity of these vasospastic attacks by relaxing blood vessels. Post traumatic stress disorder; Prazosin is utilized in the management of nightmares linked with Posttraumatic stress dsorder. Alpha blockers can be used for purposes other than its intended use to help kidney stones pass. They can also help those who have trouble urinating by relaxing the smooth muscles of the bladder. Prazosin is utilized in the management of nightmares linked with PTSD and as an adjunctive treatment for pheochromocytoma. Dibenzyline is also used to help treat pheochromocytoma. Tamsulosin can help you pass kidney stones. Side effects of alpha blockers Orthostatic Hypotension: It is a condition in which a severe and sudden fall of blood pressure occurs, when a person stands up from a resting posture. It usually appears after first dose or when dose is increased. To minimize this effect and any injury of fall, it is better to take alpha blockers at night. Nasal Congestion alpha blockers block α receptors present at nose, cause increased blood flow (vasodilatation) and nasal congestion or nasal stuffiness. it is a rare and minor side effect. Sexual Dysfunction: This is a common and reversible side effect with drugs like tamsulosin and silodosin that are used for BPH. It is distressing for patients and need to discuss with a healthcare professional. Other side effects like edema, abnormal fluid retention may appear in the treatment of BPH. Intraoperative Floppy Iris Syndrome: this rare side effect may appear in people who are taking tamsulosin and at the same time undergoing cataract surgery. The iris of the eye becomes floppy and billows out during surgery. All alpha-blockers can cause IFIS, one must inform ophthalmologist before surgery. Common side effects include dizziness, fatigue, palpitations and tachycardia what are the Precautions Liver and Kidney Disease. in case of renal & liver impairment dose must be reduced as per severity of impairment. Cataract Surgery: All alpha-blockers can cause (Intraoperative Floppy Iris Syndrome) IFIS, one must inform ophthalmologist before surgery. Pregnancy or nursing; Most alpha blockers should be taken with caution during pregnancy because there isn’t enough human data to adequately assess the danger. The only drug in this class that has more benefits than hazards is phenoxybenzamine. There isn’t enough information on the risks to babies or the effects on milk production, therefore breastfeeding can be continued. Children; Alpha blockers are applicable in pediatric patients for multiple diseases. Prazosin is utilized in the management of nightmares linked with PTSD and as an adjunctive treatment for pheochromocytoma. Dibenzyline is also used to help treat pheochromocytoma. Tamsulosin can help you pass kidney stones. Older adults’ Alpha blockers are applicable for the
Beta Blockers: Effective Antihypertensive Drugs
Beta blockers are also known as β-adrenergic receptor antagonists or blockers. They are effective antihypertensive drugs used to treat hypertension, anxiety, cardiac arrhythmia (irregular heartbeat) and other associated cardiovascular conditions. This document gives a brief information on mechanism of action, therapeutic use, precautions or contraindications and side effects of beta-blockers. Understanding of these aspects will be helpful bot only for healthcare professionals but also for patients to ensure safe and effective utilization of these medications. European Society of Hypertension (ESH) guidelines; Recent (2023) guideline from the European Society of Hypertension (ESH) add β-blockers in the group of effective antihypertensive agents that can be used as first line protocol suitable for initiation of antihypertensive pharmacotherapy. Moreover, can be used in combination with other antihypertensive agents. It is in contrast to the 2018 edition of ESH guidelines. The ESH guideline also recommends the use of β-blockers for patients having resting heart rate (>80 bpm); high resting heart rate is a sign of sympathetic overactivity may lead to the of adverse cardiac remodeling in the setting of hypertension and heart failure. It can be given alone as monotherapy or in combination also. When β-blocker is prescribed, with dihydropyridine calcium channel blocker as combination regimen, these agents reduce both peripheral and central BP. Various studies have shown that the burden of premature morbidity and mortality associated with uncontrolled hypertension, especially strokes can be reduced by combination therapy. What is the Mechanism? Beta-blockers are the competitive antagonist of beta-adrenergic receptors (sympathetic nervous system). they block the action of epinephrine and norepinephrine at beta-adrenergic receptors. These beta-adrenergic receptors are located mainly in the smooth muscles of heart, kidneys, arteries and airways. β1 Receptor Blockade: Blockage of β1 receptors in the heart decrease heart rate, contractility, and cardiac output. It reduces the workload on the heart and normalize blood pressure. these drugs also inhibit the secretion of renin by blocking β1 receptors in the kidneys, a hormone that helps to maintain blood pressure regulation. β2 Receptor Blockade: Bronchoconstriction occurs due to the blocking of β2 receptors cited at the lungs. Avoid the use of non-selective beta-blockers in patients with asthma or chronic obstructive pulmonary disease. some β2 receptors are also situated at blood vessels, and their blockade can lead to vasoconstriction. Classification of Beta Blockers Beta blockers are basically classified according to their activity on adrenergic receptors β1, β2, and β3 receptors, that are as follows: β1 Blockers al; the other name of cardio selective beta blockers. they are mainly found in the heart and kidneys. The most common drugs are metoprolol, atenolol, and bisoprolol. β1 and β2 Blockers also known as non-selective beta blockers as they block the activity of both receptors β1 and β2. Examples are propranolol, nadolol, and timolol. Alpha- and Beta-adrenergic receptor blockers: exert action by blocking both alpha and beta-adrenergic receptors. Examples include labetalol and carvedilol. These drugs are newer and more effective in youngers and lowers high blood pressure that is linked to stress or anxiety. β-Blockers with Intrinsic Sympathomimetic Activity: Few β blockers have Intrinsic sympathomimetic activity (ISA), an activity in which a drug can exhibit both agonist and antagonist properties at a given beta receptor depending on concentration. examples are penbutolol, oxprenolol, pindolol etc. Lipid-soluble beta blockers that can cross blood brain barrier e.g. Propranolol, Metoprolol Water-soluble; that has les CNS effects e.g. Atenolol, Nadolol Indications; Hypertension; Beta-blockers are effective antihypertensive drugs especially in younger patients and those with elevated sympathetic activity. in combination therapy beta blockers reduce both peripheral and central blood pressure. Angina pectoris’ beta-blockers lower myocardial oxygen demand and relieve chest pain due to angina. Heart failure: Some beta-blockers reduce the excessive sympathetic stimulation and improve the survival rate from heart failure. (Bisoprolol. carvedilol, atenolol) Arrhythmias: Beta-blockers help to manage heart rhythm by decreasing the heart rate and the excitability of cardiac tissue (esmolol, sotalol) Glaucoma: Some beta-blockers reduce intraocular pressure in glaucoma patients, Timolol is applied topically to treat glaucoma. Migraine prevention: propranolol & timolol are used prophylactically & treatment of migraine headaches. Anxiety symptoms; beta blockers are used for the symptomatic treatment of anxiety like palpitations and sweating. latest beta-blockers like nebivolol and carvedilol are more effective with fewer side effects. Hyperthyroidism beta blockers are used for the symptomatic treatment of hyperthyroidism like rapid heart rate and severity of tremors Akathisia; a movement disorder often associated with the use of antipsychotics (propranolol, metoprolol) Side Effects Central nervous system-associated side effects Fatigue or tiredness, confusion, nightmare, restlessness. hallucination, depression, insomnia, Parkinsons disease, psychosis Orthostatic or postural hypotension GIT nausea, vomiting, diarrhea Alteration of glucose & lipid metabolism (β1-blockers) Respiratory bronchospasm. dyspnea especially in asthma or COPD (more common with non-selective beta-blockers), Electrolyte disturbances; Hyponatremia, hyperkalemia (beta-1 receptor) long term side effects of beta blockers include Cold Extremities, Erectile Dysfunction, insomnia or sleep loss, difficulty to concentrate or focus, frequent mood changes, short term memory loss, a little weight gain of about 2-4 pounds. Precautions and Contraindications; It is absolutely contraindicated in hypotension, Bradycardia, cardiogenic shock, acute bronchitis, bronchospasm, Dose; Doses depend on various factors like medical condition, patient’s demographics and condition of patient. some common doses along with drugs are as Metoprolol tartrate: 25–100 mg orally 12hourly (can also be given IV, 100 mg daily in single or divided doses) Metoprolol succinate tablets/ capsule (extended-release): 25–200 mg once daily for both adults & children orally Atenolol: 25–100 mg once daily for Hypertension, angina, arrhythmias Propranolol: 40–80 mg 2-3 times a day (or extended-release 80–160 mg once daily) Timolol gel & eye drops Labetalol is the beta blocker that can be used in pregnancy induced hypertension. 0.004% of the original dose is secreted in milk, so nursing mothers should consult health care professionals. FAQ What are beta blockers? Beta blockers are the medications that lowers blood pressure, heart rate & other cardiovascular issues by blocking beta adrenergic receptors. they are used to treat many conditions like chest pain due to angina, migraine, anxiety, cardiac arrhythmia etc. Which beta blocker is best prescribed in younger people? It depends on medical
ACE inhibitors (Angiotensin-converting enzyme inhibitors)

ACE inhibitors (angiotensin-converting enzyme inhibitors) are a type of medicine that is mostly used to treat hypertension and heart diseases by relaxing blood vessels. ACE inhibitors blocks the activity of angiotensin-converting enzyme, which do not allow the conversion of angiotensin 1 into angiotensin 11. Moreover it also increases the levels of a peptide bradykinin that lowers blood pressure by opening blood vessels. All of the ACE inhibitors are available in oral dosage form except enalapril, that is available oral & intravenous injectables. FDA has approved ten angiotensin-converting enzyme inhibitors till date . Captopril was the first approved in 1981 by FDA for hypertension. Others are Enalapril, Lisinopril, Ramipril, Trandolapril, foscinopril, perindopril, quinapril, benazepril moexipril. On the basis of the chemical structure, angiotensin-converting enzyme inhibitors can be classified into three groups. yjat are Sulfhydryl-containing ACE inhibitors (Captopril) Phosphorus-containing ACE inhibitor (Fosinopril) Dicarboxylic-containing ACE inhibitors (Enalapril, Lisinopril etc) Mechanism of action Primary mode of action of angiotensin-converting enzyme inhibitors involves the suppression of the angiotensin-converting enzyme (ACE), which is necessary for the renin-angiotensin-aldosterone system. ACE inhibitors (angiotensin-converting enzyme inhibitors) blocks the conversion of angiotensin I angiotensin II. Angiotensin II is a strong vasoconstrictor that elevates blood pressure by making blood vessels smaller. ACE inhibitors controls blood pressure and enables the heart to work less by reducing the levels of angiotensin II. The reduced levels of angiotensin II opens up blood vessels, lowers blood pressure and makes the heart work less. ACE inhibitors (angiotensin-converting enzyme inhibitors) also lowers the secretion of aldosterone from adrenal glands. It makes the body hold onto less sodium and water and lowers blood volume and pressure. ACE inhibitors also inhibits the metabolism or breakdown of a peptide named bradykinin that lowers blood pressure by opening blood vessels. However the higher levels of bradykinin may create side effects like hypotension, dry cough, electrolyte imbalance or angioedema. Many drugs belong to this group. however differ a little in mechanism of action, the side effects they cause. All work much the same to lower blood pressure and protect the heart and kidneys. Indications For the treatment of high blood pressure in adults the Eighth Joint National Commission (JNC8), published evidence-based guidelines in 2014. These guidelines recommended ACE inhibitors as one of the four drug classes that can be used as initial therapy in hypertension. According to the American Heart Association/American College of Cardiology (AHA/ACC) and the European Society of Cardiology (ESC) guidelines 2023, angiotensin-converting enzyme inhibitors can be used as first-line antihypertensive protocol, preferably for the patients suffering with chronic cardiovascular diseases & diabetes mellitus. ACE inhibitors reduces the progression of disease nephropathy in Type 1 (insulin-dependent diabetes mellitus) and greatly lower the risk of death, dialysis, and transplantation. ACE inhibitors stop microalbuminuria from getting worse and turning into overt proteinuria. They also stabilize kidney function in people who have never been treated before and have compromised kidney function. Heart attack or myocardial infarction left ventricular systolic dysfunction Adverse Effects Common Adverse Effects; Dry cough, headache, fatigue, weakness, diarrhea, nausea, dizziness, Hypotension ACE inhibitor-induced dry non productive cough is more common among women than men. Reduced glomerular filtration rate GFR, & higher serum creatinine is observed in approximately 30%. It become more significant when diuretics and NSAID s are administered along with ACE inhibitors (angiotensin-converting enzyme inhibitors). One-fifth of the patients suffering with renal artery stenosis may develop elevated levels of BUN in blood urea nitrogen and creatinine levels. This decline in renal function is reversible & stabilizes within 2-4 weeks. Angioedema, most significant adverse effect that can affect any part of the body however tongue, glottis or larynx mostly effected & cause airway obstruction. Rate is high in African-American population. Many drugs like epinephrine. diphenhydramine, methylprednisolone & bradykinin blocking agents can be used. However in case of airway compromise , the airway along with an endotracheal tube is applied that allows ventilation. Hyperkalemia especialy Cholestatic jaundice or hepatitis or hepatic necrosis in rare cases Although the efficacy of Angiotensin receptor blockers (ARBs) & ACE inhibitors are similar but later has a higher incidence of side effects like cough and angioedema. this is the reason that some clinicians prefer to prescribe ARBs. over angiotensin-converting enzyme inhibitors. Hematologic disorders like neutropenia, agranulocytosis and other blood dyscrasias may occur. Precautions to use ACE inhibitors (angiotensin-converting enzyme inhibitors) Concomitant administration of ACE inhibitors and co-trimoxazole may cause mortality (sudden death) due to hyperkalemia. ACE inhibitors are contraindicated in patients with a history of angioedema or hypersensitivity. Monitor if signs of angioedema appear, like swelling of the face, lips, tongue, or throat, stop its use & seek immediate medical attention. It should not be given to patients already taking a direct renin inhibitor such as aliskiren. It should not be given to patients cardiac outflow obstruction It should not be given to patients with hypovolemia or dehydration ACE inhibitors should not be given during pregnancy due to the risk of fetal harm as it may cause congenital malformations, neonatal death or still birth, . Women planning to conceive or who become pregnant should consult physician prior use. The combination therapy of ACE inhibitors with other antihypertensive drugs especially ARBs & potassium-sparing diuretics can worse renal indices, hypotension and life-threatening hyperkalemia. Avoid if you have a known allergy to ACE inhibitors. High potassium levels or creatinine or decreased glomerular the drug needs to be adjusted accordingly or discontinued. Dosage form & Dose All of the ACE inhibitors are available in oral dosage form except enalapril, that is available oral & intravenous injectables. FDA has approved ten angiotensin-converting enzyme inhibitors till date . Captopril was the first approved in 1981 by FDA for hypertension. all have some differences regarding its uses , mechanism or side effects but they all work the same to decrease blood pressure and protecting the heart and kidneys. Some doses of ACE inhibitors for hypertension are as follow Captopril: Tab 25 mg. start dose 12.5–25 mg bid-tid with a maximum daily dose of 150mg Enalapril: Tab 5 mg. initial dose 5 mg , a maximum daily dose of 40 mg
The Role of Public Health Policies in Controlling Non-Communicable Diseases
Non-communicable diseases (NCDs) such as heart disease, diabetes, and cancer are major health challenges worldwide. Unlike infectious diseases these diseases are caused by a combination of the following; lifestyle, environmental and genetic factors. With an increasing global burden of NCDs, the presence of public health policies is essential in curbing the epidemic, as well as limiting its effects. In this article, we’ll explore the role of public health policies in tackling non-communicable diseases, focusing on their preventive measures, strategies, and the significant role organizations like DFD play in improving public health outcomes. What Are Non-Communicable Diseases (NCDs)? Non-communicable diseases are a group of medical conditions that are not transmitted from person to person. Rather, they come about due to the course of time and are often as a result of poor eating habits, insufficient physical activities, use of tobacco, and the intake of alcohol in amounts that are beyond normal. The typical NCDs are: They have been responsible for causing most deaths in the world, and pose a great problem to the health system, economy, and the quality of life of people. Why Public Health Policies are Essential when it comes to NCD Control? Public health policies are essential in controlling non-communicable diseases for several reasons. The application of effective policies to the prevention of NCDs focuses on eliminating the causes of them, encouraging a healthier lifestyle, and decreasing the general prevalence of the health issues. It is because of this that such policies are essential: 1. Encourage Healthy Life Style Decisions Public health policies aimed at controlling non-communicable diseases focus on promoting healthier lifestyle choices. Governments can infer and avoid the development of such diseases by promoting exercise, nutrition, and by quitting smoking. As an example, the marketing of unhealthy food, tobacco, and alcohol can be an important approach since such policies can diminish the consumption of these risk factors considerably. DFD is supportive of such policies so that the health outcomes of populations are improved. 2. Increase the Participation of People into Public Awareness Effective methods to curb Ncds are educational and awareness programs that can also be considered to be one of the most potent ways to control Ncds. Included in the public health policies are the awareness programs on the danger of smoking, poor diets, and a sedentary lifestyle. Through these campaigns, people are informed about how to prevent non-communicable diseases, leading to better health choices. As an illustration, to restrain Ncds, Dfd has been determined to educate people on the significance of consistent exercise and healthy diets through its mission statement. 3. Health Services and Early Detection Good public health policies make healthcare services such as screenings and diagnostic tools available to all people. Diagnosing NCDs, including cancer and diabetes at an early stage in one or another can save a lot and positively impact diseases as a whole. Governments usually partner with organisations, such as DFD, by making sure that poor groups can afford health services, which will help them to detect their possible NCDs in early stages of development. 4. Risk factor’s regulation Another important feature of the public health policies lies in the regulation of the risk factors of NCDs. Taxation of the sweetened beverages, ad ban of the tobacco products, alcohol sale norms are some of the measures that can be dictated by the government to curb the propensity of engaging in the behaviors that lead to the development of the NCDs. Policies aimed at creating “healthier environments” are key to reducing the risk of non-communicable diseases, and DFD advocates for such regulations globally. Effective Strategies for Controlling Non-Communicable Diseases A mixture of various methods usually works as a public health policy to regulate NCDs. The best of them are the following: 1. Prevention and Health Promotion Programs 2. Better access to Healthcare 3. Health Education Advocacy 4. Data-collection and Surveillance Surveillance and data-collection National insurance surveillance and data-collection What can be done to have a better future through NCD prevention? This is because a healthier future cannot be reached without the community of government, healthcare providers and individuals working to make it happen. The following are some tips of how to move on: Frequently asked questions (FAQs) 1. What are the most common non-communicable diseases? The most common non-communicable diseases include cardiovascular diseases, diabetes, chronic respiratory diseases, and cancer. These are lifestyle-related diseases, commonly linked to diet, physical activity, and smoking. 2. What role can be played by the public health policies to curb NCDs? Public health policies can help by promoting healthy lifestyles, regulating risk factors, improving healthcare access, and raising awareness about the prevention of non-communicable diseases. 3. How does DFD help with NCDs control? DFD supports policies that reduce NCD incidence, promotes awareness on healthy lifestyles, and collaborates with governments and health institutions to improve healthcare affordability. 4. How do non-communicable diseases impact society? Non-communicable diseases put heavy pressure on healthcare systems, harm economies, and affect individuals by causing premature deaths, disabilities, and costly treatments — reducing overall societal welfare. 5. Can non-communicable diseases be prevented? Yes, they can be prevented with lifestyle changes such as healthy eating, regular physical activity, quitting smoking, and limiting alcohol. Public health policies play a key role in supporting these changes.
Amlodipine besylate
Amlodipine besylate is a common calcium channel blocker (CCB) that is mostly used to treat high blood pressure and chronic stable angina (chest discomfort). It is a calcium antagonist and belongs to the dihydropyridine class, which means it relaxes blood vessels and makes blood flow better. It was approved for medical use in 1990 and included in the essential medicine list of WHO. According to a report of 2022, it was the fifth most commonly prescribed medication for hypertension in the United States of America. Amlodipine is a good choice for treating high blood pressure because it has a lengthy half-life of 30 to 50 hours and only needs to be taken once a day. The bioavailability of amlodipine besylate is 64% to 90% & plasma concentrations is achieved in 6 to 12 hours. Amlodipine is metabolized by the liver to inactive metabolites and excreted by kidneys. Mechanism of action of Amlodipine involves a number of important steps Being peripheral arterial vasodilator, it stops calcium from getting into smooth muscle in arteries, causes vasodilation, which lowers systemic vascular resistance and blood pressure. By stopping calcium from getting into cells, amlodipine opens up coronary arteries, which makes it easier for the heart to get oxygen, especially in people with vasospastic angina. It binds to the alpha1 subunit of L-type calcium channels, prevent its opening. It reduces the entry of calcium ions and modifies the contractility of the heart and smooth muscle. All of these mechanisms work together to make amlodipine effective for treating high blood pressure and angina. What Amlodipine besylate is used for High blood pressure (hypertension) Reduces peripheral vascular resistance by relaxing the smooth muscle in the arteries, which lowers blood pressure. By opening up the coronary arteries, it increases blood flow to the heart and lowers the number of angina episodes. Chronic stable angina (due to physical or emotional stress) Vasospastic angina Often used as a first-line treatment, either by itself or with additional antihypertensive medications. Helps to stop spasms in the coronary arteries that cause chest discomfort. A new study suggests that amlodipine, can help to manage ADHD symptoms as it significantly reduced hyperactivity when used on rats and zebrafish. Dose & dosage form of Amlodipine besylate It is available in oral dosage form i.e. Tablets of 2.5mg, 5 mg and 10 mg. In adults: Initially, a dose of 5 mg/day is recommended once a day & should not exceed 10 mg/day. In children and adolescents (6 to 17 years of age), the initial dose of 2.5 mg once a day is the recommended dose. Children under six years initial dose is 0.05-0.1 mg/kg/day & can be raised a maximum dose of 0.6 mg/kg/day after a week. People over 65 or with liver problems may start with 2.5 mg/day. For angina patients, first dose is 5 mg once a day. The maintenance dose will be 5 to 10 mg once a day, with a maximum dose of not more than 10 mg per day. Amlodipine besylate can be taken with or without food, but better to take at same time to get best results. It should be taken with a glass of water. Warnings and Things to Avoid Amlodipine besylate is usually well-tolerated, however there are several things you should do to be safe Hypotension (low blood pressure) can cause blood pressure to drop too much, especially in patients who are low on volume. Severe Aortic Stenosis: Be careful when using it because it can lower blood flow to the heart. Liver damage: You may need to change the dose since your metabolism is slower. Heart Failure: Be careful when giving Calcium channel blockers to those with heart failure, as they may make symptoms worse in some circumstances. Pregnancy (Category C): Only use if the benefits are greater than the hazards. Breastfeeding: A little quantity of the drug comes out in breast milk. Talk to your doctor before using it. Keep all medication out of sight and reach of children as many containers are not child-resistant. and away from light, excess heat and moisture Always lock safety caps. Place the medication in a safe location – one that is up and away and out of their sight and reach. Dispose of unneeded medications side effects of Amlodipine besylate Most side effects are mild to moderate, but some may need medical help Common side effects of amlodipine besylate include peripheral oedema (which is swelling in the ankles and feet) migraines, hypotension etc Some adverse effects are related to dose like dizziness, weakness, palpitations, and hot flushes. Rare effects include jaundice, pancreatitis, hepatitis or cholestasis and high levels of transaminases. Allergic reactions, erythema, pruritus associated with amlodipine that disappear with the discontinuation of treatment. Chest discomfort that gets worse (not often, but can happen in angina patients) Amlodipine-associated gingival overgrowth. symptoms of overdose may include dizziness, tachycardia, fainting & severe low blood pressure. It can be treated with fluid replacement and maintaining glucose levels. Need to monitor patient s vital signs, respiratory system function, blood glucose levels, renal function and urine output. Interactions between drugs Amlodipine besylate can change how other drugs work, when taken together: Amlodipine may raise the levels of simvastatin (don’t take more than 20 mg/day of simvastatin). Strong CYP3A4 inhibitors, such ketoconazole, itraconazole, and clarithromycin, are: Increase the amount of amlodipine in your body, which raises the chance of negative effects. Other antihypertensives, like beta-blockers, ACE inhibitors, and diuretics, may make the blood pressure-lowering effects stronger, which raises the risk of low blood pressure. Grapefruit juice may help the body absorb amlodipine better, which can raise blood levels. If you are taking other medicines either prescribed or over the counter, inform your doctor and pharmacist. Dose of amlodipine may need to change, or careful monitoring may be required.You must inform your healthcare professional if you ever had heart or liver disease. Amlodipine besylate is a good and often given medicine for high blood pressure and angina. It just needs to be taken once a day and is
Calcium Channel Blockers (CCBs)
Calcium channel blockers are a type of antihypertensive medicine that stops calcium ions from getting into cardiac and smooth muscle cells. This causes blood vessels to widen, the heart rhythm to slow down, and blood pressure to drop. They are often used to treat high blood pressure, chest pain, and some types of arrhythmias. Calcium channel blockers (CCBs) work especially well to make large blood vessels less stiff. This stiffness is a typical cause of high systolic blood pressure in older people. Calcium channel blockers became quite popular in the 1960s. This group of drugs was discovered in the lab of German pharmacologist Albrecht Fleckenstein in 1964. Classification of Calcium channel blockers They are of two types, known as dihydropyridines and non-dihydropyridines. Dihydropyridines Mainly it causes vasodilation, decreases Blood Pressure, may cause reflex tachycardia. This CCB class can be easily recognized by the suffix -dipine .Examples include Amlodipine, Nifedipine, Felodipine, Nimodipine etc. Non-Dihydropyridines; its primary action is cardiac depression, decreases heart rate & contractility, produce anti-arrhythmic effect. Examples include Verapamil, Diltiazem Mechanism of Action Calcium channel blockers stop L-type voltage-gated calcium channels from working in the smooth muscle of blood vessels, heart muscle cells, and nodal tissue. Vascular Action: Stops calcium from getting into smooth muscle in arteries, which causes vasodilation, which lowers systemic vascular resistance and blood pressure. Cardiac Action (non-Dihydropyridines): Lower calcium entrance into SA and AV nodes, which slows conduction, lowers heart rate, and lowers myocardial contractility. Therapeutic Uses The FDA has approved different uses for each medicine of Calcium channel blockers. These medicines are commonly prescribed for the treatment of Hypertension (especially in elderly and Black patients) Arrhythmias. supraventricular tachycardias used to regulate / manage cardiac beats (Verapamil/Diltiazem) Angina Pectoris treat chest pain due to angina pectoris Raynaud’s phenomenon Hypertrophic cardiomyopathy (a disease in which the heart muscle gets thickened) Migraine prophylaxis (off-label) Adverse effects. Dihydropyridines. cough Peripheral edema (Swelling in the legs and feet) Headache, flushing, fatigue, heartburn Reflex tachycardia Hypotension can worse proteinuria in neuropathic patients Non-Dihydropyridines Bradycardia Constipation (especially due to verapamil) AV block Worsening heart failure Drug interactions Calcium channel blockers including Dihydropyridines & Non dihydropyridines are metabolized in liver through cytochrome P450 enzyme system, making them prone to several clinically significant drug interactions. Some common & general drug interactions are as follow Beta-blockers – CCBs (esp. with non-DHPs) may lead to additive cardiac depression. Concomitant administration will increase the risk of bradycardia, hypotension & heart block. better to use some other antihypertensive or monitor closely. Digoxin-CCBs (with verapamil/diltiazem) Inhibits renal clearance of digoxin. It increases digoxin toxicity that can be characterized by nausea, arrhythmias etc. need to monitor serum levels. CYP3A4 inducers (e.g., rifampin, phenytoin, carbamazepine)-CCBs when given together lead to increased metabolism of CCBs, decrease the efficacy of CCBs. Consider dose increase or use alternate. Statins -CCBs (esp. simvastatin with amlodipine/verapamil), inhibits metabolism of statins that increase the risk of myopathy. it is better to limit the simvastatin dose to ≤20 mg/day with amlodipine Antiarrhythmics (e.g., amiodarone) -CCBs synergies the effects on AV conduction & increases risk of AV block, bradycardia. Monitor ECG and symptoms. Lithium & CCBs, reduce the clearance of lithium, may lead to lithium toxicity. When to administer with caution Hepatic impairment: Patients with hepatic impairment typically need to have their doses changed because these medicines are broken down in the liver. So, it is best to look up the information on the individual agent in the package insert or other trustworthy sources. Renal impairment: Most of the time, patients with renal impairment don’t need to change their dose. But better to get guidance from doctors should check the renal dose. Pregnant women: Limited data from human research indicate that fetal damage is generally not anticipated with either class of calcium channel blockers (CCBs). When administering CCBs on pregnant women, doctors should think about the risks and benefits. Breastfeeding women: There is not enough data from human research to say that either class of CCBs would hurt babies. However, there is no data to determine how these medications affect milk production. Older patients: CCBs are excreted more slowly in senior individuals, therefore be careful with those who have liver problems. Conclusion Calcium channel blockers are essential agents in the management of hypertension, particularly in elderly patients and those with specific comorbidities such as angina or arrhythmias. Due to their favorable safety profile and robust outcome data, these agents remain the preferred choice for first-line treatment, frequently utilized in combination regimens to achieve optimal control. FAQ 1. What are calcium channel blockers and what is their mechanism of action? Calcium channel blockers are medications that reduces muscle contraction, vasodilation, lower blood pressure and in some cases heart rate also by blocking L-type calcium channels in heart and blood vessels. 2. What conditions are calcium channel blockers used to treat? Hypertension (especially in elderly and Black patients), Arrhythmias. supraventricular tachycardias used to regulate / manage cardiac beats (Verapamil/Diltiazem), Angina Pectoris treat chest pain due to angina pectoris, Raynaud’s phenomenon, Hypertrophic cardiomyopathy (a disease in which the heart muscle gets thickened) & Migraine prophylaxis (off-label) 3. What are the common side effects of calcium channel blockers? Peripheral edema (Swelling in the legs and feet), Headache, flushing, Reflex tachycardia, Hypotension, Bradycardia, Constipation (especially due to verapamil), AV block etc..
Classification of Antihypertensive drugs
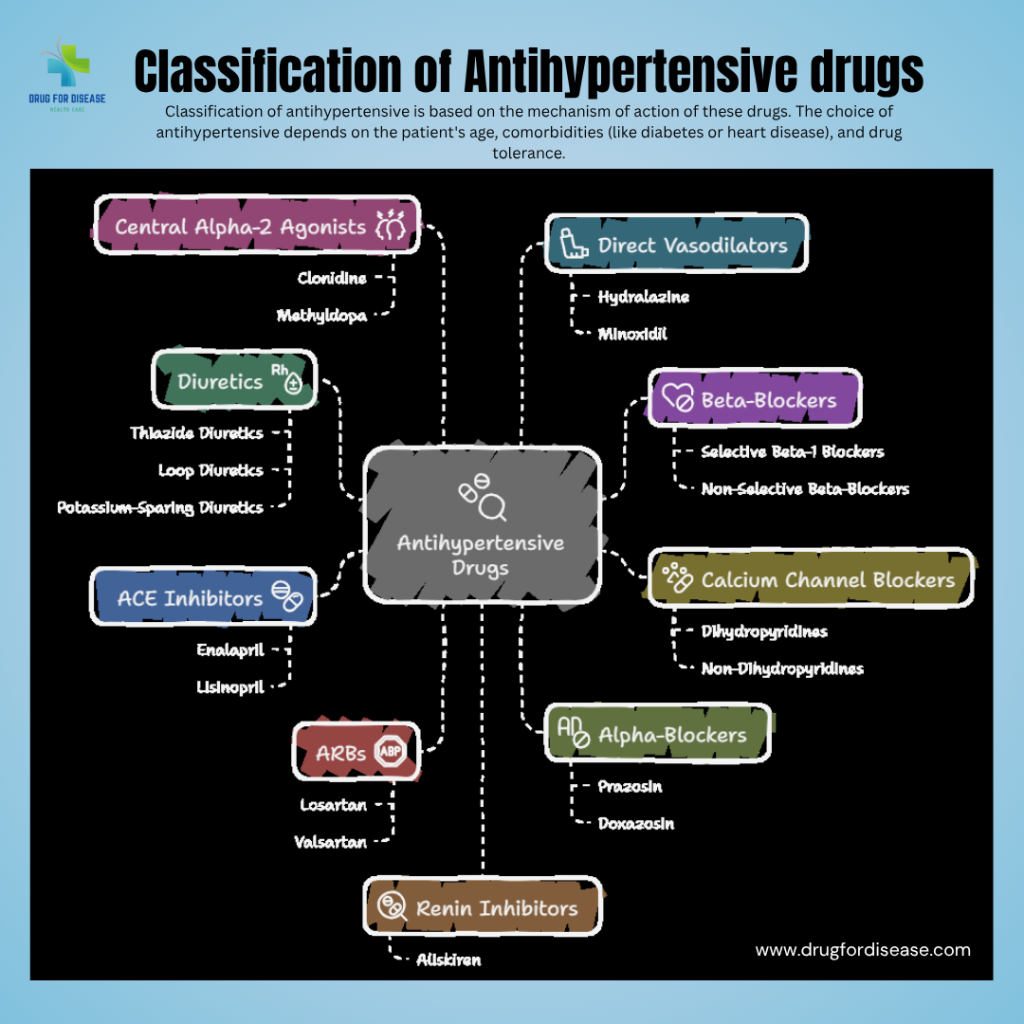
Antihypertensive drugs are medicines that help to lower high blood pressure (hypertension). They employ diverse physiological approaches to control blood pressure and reduce the chances of complications such as heart attacks, strokes, and effects on kidney. Classification of antihypertensive is based on the mechanism of action of these drugs. groups are as follow 1. Diuretics; also known water pills Increased renal excretion of sodium and water—causes reduction in blood volume. increase excretion of sodium and water by the kidneys, reducing blood volume. Diuretics are are considered as first line treatment of hypertension. Examples: Thiazide Diuretics: basic site of action is distal convoluted tubule of the nephron. e.g. Hydrochlorothiazide, Chlorthalidone Loop Diuretics; site of action is ascending loop of Henle. e.g. Furosemide Potassium-sparing Diuretics; inhibit Na reabsorption at the collecting tubules. e.g. Spironolactone, Amiloride, Triamterene 2. Beta-Blockers (β-Blockers) Decrease heart rate, cardiac output and ultimately lowers blood pressure.by blocking the effects of epinephrine and norepinephrine on beta-adrenergic receptors. Examples: Atenolol, Metoprolol, Propranolol 3. Calcium Channel Blockers (CCBs) Prevents movement of calcium into vascular smooth muscle, which leads to vasodilation and reduced heart contractility. Dihydropyridines: mainly act on blood vessels and cause vasodilation. Amlodipine, Nifedipine Non-dihydropyridines: Act on blood vessels and the heart & reduce heart rate and contractility. Verapamil, Diltiazem 4. Angiotensin-Converting Enzyme Inhibitors (ACE Inhibitors) Mechanism: Suppress the action of a vasoconstrictor — angiotensin II by inhibiting the angiotensin-converting enzyme (ACE). Examples: Enalapril, Lisinopril, Ramipril 5. Angiotensin II Receptor Blockers (ARBs) Mechanism: block the action of angiotensin II (vasoconstriction) and prevent it to bind to its receptors on vascular smooth muscle cells in various tissues. Examples: Losartan, Valsartan, Telmisartan 6. Alpha-Blockers (α-Blockers) Mechanism: Block alpha-adrenergic receptors, leading to vasodilation. Examples: Prazosin, Doxazosin 7. Central Alpha-2 Agonists Mechanism: Reduce sympathetic outflow from the brain. Examples: Clonidine, Methyldopa 8. Direct Vasodilators Mechanism: Act directly on blood vessel walls to relax and dilate them. Examples: Hydralazine, Minoxidil 9. Renin Inhibitors Mechanism: Directly inhibit renin, reducing angiotensin I and II levels. Example: Aliskiren The choice of antihypertensive depends on the patient’s age, comorbidities (like diabetes or heart disease), drug tolerance and potential adverse effects. FAQ 1. What are the most commonly used classes of antihypertensive drugs? Diuretics Beta-blockers Calcium channel blockers ACE inhibitors ARBs (Angiotensin II Receptor Blockers) Alpha-blockers 2. What things you must consider while choosing the right class of antihypertensive drug for a patient? Answer:Choice depends on factors like age, ethnicity, comorbidities (e.g., diabetes, heart failure, CKD), and drug tolerance. For example, ACE inhibitors are preferred in diabetics, while calcium channel blockers work well in elderly and Black patients. 3. Can different classes of antihypertensive drugs be used together? Answer:Yes, combining drugs from different classes (e.g., ACE inhibitor + diuretic or ARB + calcium channel blocker) is common for better blood pressure control and reduced side effects.
Hypertension (high blood pressure)
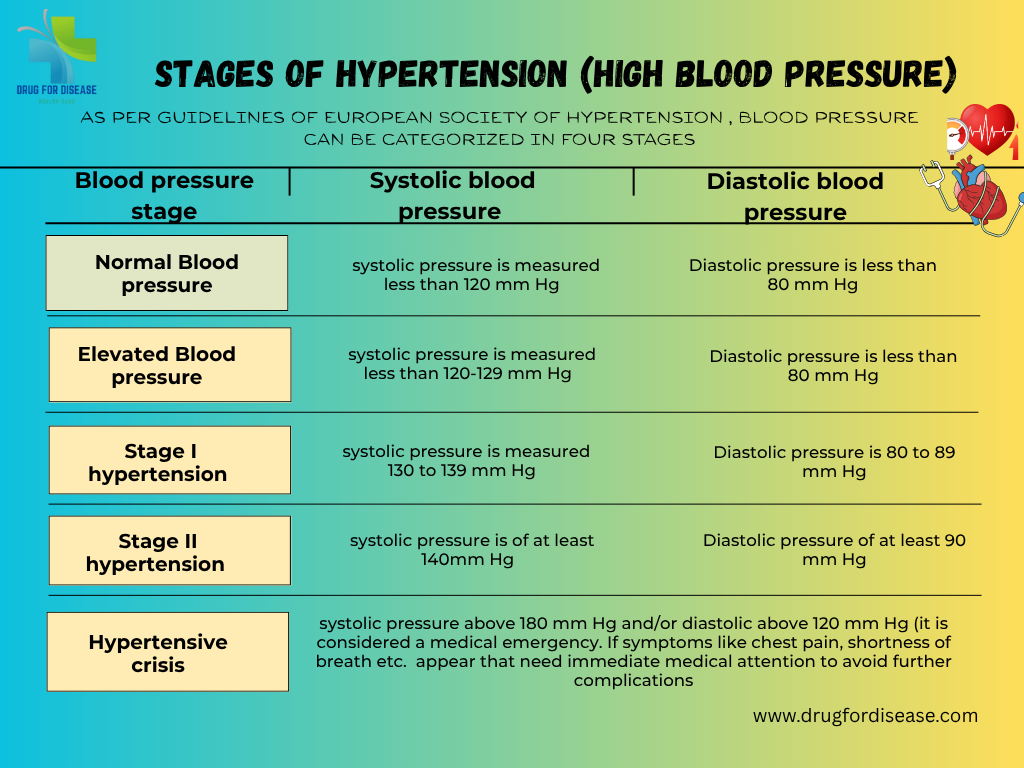
Hypertension or high blood pressure is the most common non communicable disease that appears when the force (pressure) of blood against the artery walls is continuously high. Or in other words consistent raised arterial pressure is termed as hypertension. How to take readings of hypertension Hypertension or high blood pressure is measured by two values that are systolic pressure & diastolic pressure. Systolic blood pressure represents the pressure of blood in arteries when heart beats & diastolic blood pressure is the pressure of blood is on artery walls when the heart muscle rests between beats. A normal blood pressure value is 120/80 mmHg. Hypertension or high blood pressure is usually diagnosed when blood pressure consistently exceeds 130/80 mmHg. Globally1.28 billion adults between the age of 30–79 years are suffering from hypertension. About two-thirds of hypertensive cases belong to low- and middle-income countries. It is the major cause of premature mortality (WHO, 16 March, 2023). Stages of Hypertension or high blood pressure As per European Society of hypertension guidelines, blood pressure can be categorized in four stages Normal Blood Pressure: systolic pressure is less than 120 mm Hg while diastolic is less than 80 mm Hg Elevated Blood pressure: systolic pressure of 120-129 mm Hg and diastolic less than 80 mm Hg, need to consult health care professional to manage the condition. Stage 1 Hypertension: systolic pressure of 130 to 139 mm Hg or diastolic of 80 to 89 mm Hg. It can be managed by lifestyle changes and medication. Stage 2 Hypertension: systolic pressure of at least 140 mm Hg or diastolic of at least 90 mm Hg or above. Hypertensive crisis: systolic pressure above 180 mm Hg and/or diastolic above 120 mm Hg (it is considered a medical emergency. Following symptoms may appear, that need immediate medical attention to avoid further complications chest pain, shortness of breath, difficulty in speaking, numbness, weakness, blurred vision etc. Types of Hypertensions (high blood pressure) Hypertension or high blood pressure is basically classified into two major types, that are Primary /Essential Hypertension; It is the most common type, affecting between 90 to 95 percent of people. It develops slowly over time and has no known cause, but linked to behavioral factors, genetic, environmental factors, diet, smoking, excessive salt intake, less physical activity etc Secondary Hypertension Secondary Hypertension or high blood pressure is affecting 5–10% percent of people worldwide. It occurs suddenly and is due to an underlying medical condition or conditions like adrenal gland tumors, thyroid problems, stroke, kidney failure, birth control tablets or medicines etc. Secondary hypertension is more prevalent in younger people & 30% of people have an age of 18 to 40 years. Other Subtypes of hypertension include Isolated Systolic Hypertension Mostly older people suffer with isolated systolic hypertension. Blood pressure ranges from 140- 90mmHg systolic pressure and diastolic pressure respectively. Malignant Hypertension (Hypertensive Emergency Blood pressure rises quickly and severely (typically >180/120 mmHg. It may cause damage to one or more organs like kidney, lungs, brain etc. symptoms.like confusion, anxiety, drowsiness, chest pain, and shortness of White Coat Hypertension: Elevated blood pressure only in clinical settings due to anxiety while patient gets normal at home Masked Hypertension; It is the vice versa of above readings is normal in clinical settings but elevated at home or in daily life. Gestational hypertension Hypertension occurs in approximately 8–10% of pregnancies after 20 weeks of gestation and women have a blood pressure higher than 140/90 at two readings with at least 6 hours gap Other pregnancy related hypertension or high blood pressure are Pre-eclampsia & Eclampsia that need special care and emergency treatment. Causes & Risk Factors of hypertension or high blood pressure No physical activity unhealthy diet that are rich in salt, sugar, saturated and trans fats, carbonated drinks, etc. smoking tobacco or being exposed to secondhand smoke that may damage blood arteries and cause high blood pressure. excessive salt intake anxiety or stress Being overweight or obese Family history or genetic factors Age and sex Adrenal tumors (e.g., pheochromocytoma) Medications (NSAIDs, steroids, birth control pills Chronic kidney disease Hyperthyroidism or hypothyroidism COMPLICATIONS OF HYPERTENSION Coronary heart disease (CHD) Myocardial infarction (MI) Stroke (CVA), either ischemic or intracerebral hemorrhage Hypertensive encephalopathy Renal failure, acute versus chronic Peripheral arterial disease Atrial fibrillation Pathophysiology & Diagnosis Increased salt absorption resulting in volume expansion Increased activation of the sympathetic nervous system An impaired response of the renin-angiotensin-aldosterone system (RAAS) It can be diagnosed by routine blood pressure monitoring with electronic or manual BP apparatus sphygmomanometer, blood tests (renal function, electrolytes, lipid profile), urine test etc. Treatment Plans Lifestyle Modifications Medications: Preferred drugs are Diuretics, Calcium channel blockersm ACE inhibitors, Beta blockers Identify and treat the underlying cause Adjust or stop contributing medications Hypertension or high blood pressure is often silent but deadly. Early detection, lifestyle changes, and appropriate treatment can prevent serious complications. Everyone over the age of 30 should monitor their blood pressure regularly—even if they feel healthy.
New eye drops with oxysterol compound (VP1-001) may treat cataracts without surgery
A study from Anglia Ruskin University showed that eye drops with oxysterol compound (VP1-001) may treat cataracts without surgery. The study’s results were published on May 2nd, 2022, in the peer-reviewed journal Investigative Ophthalmology and Visual Science. A cataract is an eye disorder in which clouding of the eye lens worsens over time and disrupts the quality of vision. A cataract is a disorder in which the proteins in the lens accumulate & make a cluster or cloud. This cloud scatters light and significantly limits its transmission to the retina. Cataract is the most common cause of visual loss in the world. According to the report of WHO (10 August 2023), 17% of people are globally affected with vision impairment due to cataracts at age 40 or older. At present, cataract surgery is the only way for the treatment of cataracts. In this surgical procedure the hazy lens is replaced with an artificial intraocular lens. Including economical burdens, cataract surgery has many complications like inflammation, xerophthalmia macular oedema, and posterior capsular opacificationHowever, a few scientists at Anglia Ruskin University under the supervision of Prof. Barbara, Deputy Dean in the Faculty of Health, Education, Medicine, and Social Care, conducted optical tests on an oxysterol compound that is considered an anti-cataract drug. They prepared new eye drops that could get rid of cataracts without surgery. VP1-001 is a chemical that is in these drops. It works by repairing the protein clumps in the eye lens that make it cloudy. A single drop increased the lens’s clarity and focusing capacity when tested on mice with cataracts. The study’s results were published on May 2nd, 2022, in the peer-reviewed journal Investigative Ophthalmology and Visual Science. Outcomes of optical tests with eye drops The outcomes were good: 61% of the eyes that were treated were better able to focus due to the improvement in the refractive index profiles 46% of them became clearer and more transparent. Results: This is a huge advance since it means that some cataracts might be able to be cured with drugs instead of surgery. But the drops didn’t work on all kinds of cataracts, so additional research is needed to find therapies that work for everyone. Moreover, these drops aren’t available for individuals now. More research is needed These drops aren’t available for individuals now, but this is a big step forward, especially in countries where eye surgery is hard to get. This study is a hope towards non-surgical treatment of cataracts with the oxysterol compound (VP1-001). Cataract surgery is a safe and effective solution, as it completely replaces the clouded lens with an artificial one. The oxysterol compound (VP1-001) is still in the preclinical stage and not approved for human use. It’s under clinical trials. Moreover, safety testing will be confirmed before public availability. 📌 Published in: Investigative Ophthalmology and Visual Science (May 2, 2022) by Anglia Ruskin University Frequently asked questions 1. What are the types of cataracts? Caract can be classified by many wayss; however, it can be categorised into three types, on the basis of cloud location/formation, that are Posterior subcapsular cataract Age-related cataracts. Cortical cataracts. Nuclear Cataracts. 2. What are the risk factors of cataracts? Age is the major factor of cataracts, especially at 40 or above. other factors include diabetes, smoking, obesity, hypersensitivity, excessive exposure to sunlight, eye injury or inflammation, etc. 3. Are there any eye drops or drugs to treat cataracts without surgery? As of now (2025), there is no approved eye drop or drug that can treat or reverse cataracts without surgery, but research at Anglia Ruskin University showed that the experimental drug VP1-001 (oxysterol-based eye drops) works as an anti-cataract in animal trials. 4. What are the complications of cataract surgery? Many complications, like inflammation, xerophthalmia, and macular oedema, can occur as post-surgical conditions. 5. What is the oxysterol compound VP1-001? Oxysterol compound VP1-001, also known as compound 29, has shown a significant effect on the treatment of cataracts in a trial on mice. It reduces the opaqueness of the lens that may occur due to risk factors like ageing & mutation.
What Are Non-Communicable Diseases (NCDs)?
Non-communicable diseases are a group of medical conditions that are not transmitted from person to person. Rather, they come about due to the course of time and are often a result of poor eating habits, insufficient physical activities, use of tobacco, and the intake of alcohol in amounts that are beyond normal. These are the long-term health conditions that are driven by lifestyle or behavioural factors. A longitudinal study from 2003 to 2014 identified the spectrum and trends of non-communicable disease prevalence in inpatients of 12 hospitals in China. It is expected that by 2030, NCDs will be the main cause of death in Sub-Saharan Africa, killing more people than communicable, maternal, neonatal, and nutritional (CMNN) illnesses put together. Most common non-communicable diseases include: Cardiovascular disorders (17.9 million people died globally) Chronic respiratory diseases (9 million people died annually) Cancer (3.9 million people died annually) Diabetes (1.6 million people died annually) The above-mentioned have been responsible for about 70-80% of global morbidity & mortality, especially in the lower middle-income countries. NCDs not only burden the economy of a health system but also the quality of life of people. Cardiovascular diseases are the disorders of circulatory system, like High Blood Pressure, Peripheral Artery Disease, Rheumatic Heart Disease, stroke, etc. Chronic respiratory diseases are type of chronic diseases that appear due to the functional impairment of lungs and the respiratory system, like asthma, chronic obstructive pulmonary disease, etc. Diabetes, a metabolic condition, occurs due to high blood sugar levels. mainly of three types: Type 1 diabetes, Type 2 diabetes & gestational diabetes. Cancer occurs due to the abnormal growth of cells that develop and spread without control. Some common cancer categories are lung cancer, breast cancer, colorectal cancer, etc. Risk factors of non-communicable diseases NCDs Behavioural risk factors Genetic risk factors Environmental risk factors Metabolic risk factors Socio-demographic factors Global Effects of NCD High Mortality Rate: According to the WHO report 2021, about 43 million people die every year due to noncommunicable diseases, and 82% of the mortality data is from lower-middle-income countries. Economic Burden: NCDs put a lot of stress and burden on healthcare systems and ultimately increase health costs. Higher Healthcare Costs: A lot of budget is required for the management of chronic conditions. These noncommunicable diseases need long-term medical care, drugs, improved healthcare systems like telehealth, & human resources to address these issues, all of which will add up to a lot of money. Lower Quality of Life or Reduced Work Capacity: People suffering with chronic diseases will be less productive towards work. It’s hard to do everyday things, causes discomfort, and may lead to disability. Policies for Public Health; To effectively manage common NCDs, it is important to put preventive health programs first and improve the healthcare system. Health education programs can give people in a community the information they need to avoid getting sick and find out about it early, which could lower the number of sick people. Tobacco Control: strong measures need to be adopted to control tobacco use, like increasing taxes, declaring smoke-free areas, and efforts to raise public awareness Promoting a Healthful Diet: Food having a high quantity of salt, sugar, and saturated and trans fats is linked to obesity, type 2 diabetes, and cardiovascular conditions. Labels on food items along with nutritional value & minimum price will be helpful. Promoting Physical Activity: need to build grounds, parks, paths to improve physical activity free of cost Alcohol Control: Implement rules to discourage drinking, like taxes, age limits on the purchase & sale of alcohol, and people awareness by social media. What healthcare actions need to be taken Improving air quality by developing and implementing policies of waste management, pollution, etc. Early detection and screening Management of risk factors especially behavioural factors Access to essential medicines and technology to every person Integrated Care Models Community-Based initiatives Self-Management Education In simple words, diseases that do not spread from person to person are a big threat to the health and well-being of people all over the world. The ratio of NCDs can be decreased and the health and quality of life of people enhanced by knowing what the risk factors are, using good prevention methods, and making sure everyone has access to appropriate healthcare centres. To properly deal with this worldwide problem, governments, healthcare professionals, communities, and individuals must all work together. FAQ 1. What are the most common non-communicable diseases? The most common non-communicable diseases include cardiovascular diseases, diabetes, chronic respiratory diseases, and cancer. These are lifestyle-related diseases, and this is commonly related to such aspects as diet, physical activities, and smoking. 2. How do non-communicable diseases impact a society? Non-communicable diseases place a significant burden on healthcare systems, economies, and individuals. These cause untimely deaths, disability and treatment that is very expensive, which are all related to the overall welfare of the society. 3. What are the risk factors that can be changed? Noncommunicable diseases (NCDs) are significantly influenced by modifiable behavioural risk factors. that lifestyle changes, healthy diets, cessation of smoking & alcohol, improved physical activity, weight management, etc.

